







Statistical Bulletin 2017 — prevalence of drug use
Archived content
Prevalence and patterns of drug use in the general population (adults or school children) is assessed through surveys based on representative probabilistic samples of the whole population under study. Interview surveys are based on self-report of participants regarding present and past behaviours, personal characteristics, knowledge and attitudes regarding drugs or other health topics.
Data tables
Use the menu below to find data sets of interest.
Graphics
Click on a graphic from the thumbnails below



Methods and definitions used
The European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) general population survey (GPS) indicator focuses on estimates of the prevalence and patterns of drug use in the European Union (EU) Member States, Norway and Turkey. The EMCDDA monitors data from national and school surveys based on representative, probabilistic samples. The surveys consist of self-reported data on present and past drug use, personal characteristics, and knowledge and attitudes regarding drugs or other related topics (e.g. health topics). Metadata on factors likely to influence the interpretation, validity and reliability of the data are also collected, and the results are reported in the Data and statistics section (Statistical Bulletin) of the European Drug Report.
The EMCDDA encourages countries to harmonise their data collection and reporting (1) Nevertheless, differences in survey methodology will influence the interpretation and comparability of the results. It is important to be aware of changes in the survey methodology within individual countries when interpreting trends.
Users of the data should carefully consider the methods and definitions described below and the notes associated with the data in the Statistical Bulletin. The Handbook for surveys in the general population provides further information necessary for interpreting the data. The individual country National reports are a source of contextual and methodological information and the basis of much of the information here. All of the above are available on the EMCDDA website (see ‘Key links’ below).
Data on the prevalence of drug use should be considered within the broader range of available information. Cross-referencing between data-sets provides both additional insights and a check of validity. Prevalence estimates provide a backdrop to all of the key data-sets collected by the EMCDDA. For example, they provide information on the frequency of use of the more commonly used drugs and an indication of high-risk drug use (problem drug use (PDU) indicator), and can be compared with data on entrants into treatment (treatment demand indicator (TDI)).
Purpose and aims
General population surveys allow the prevalence of drug use to be estimated. At its simplest, the proportion of the sample declaring that they have used specific drugs is taken as an estimate of the prevalence of use within the population. Further information on the characteristics of the participants and their patterns of drug use allows the potential determinants and consequences of drug use to be investigated.
Definitions
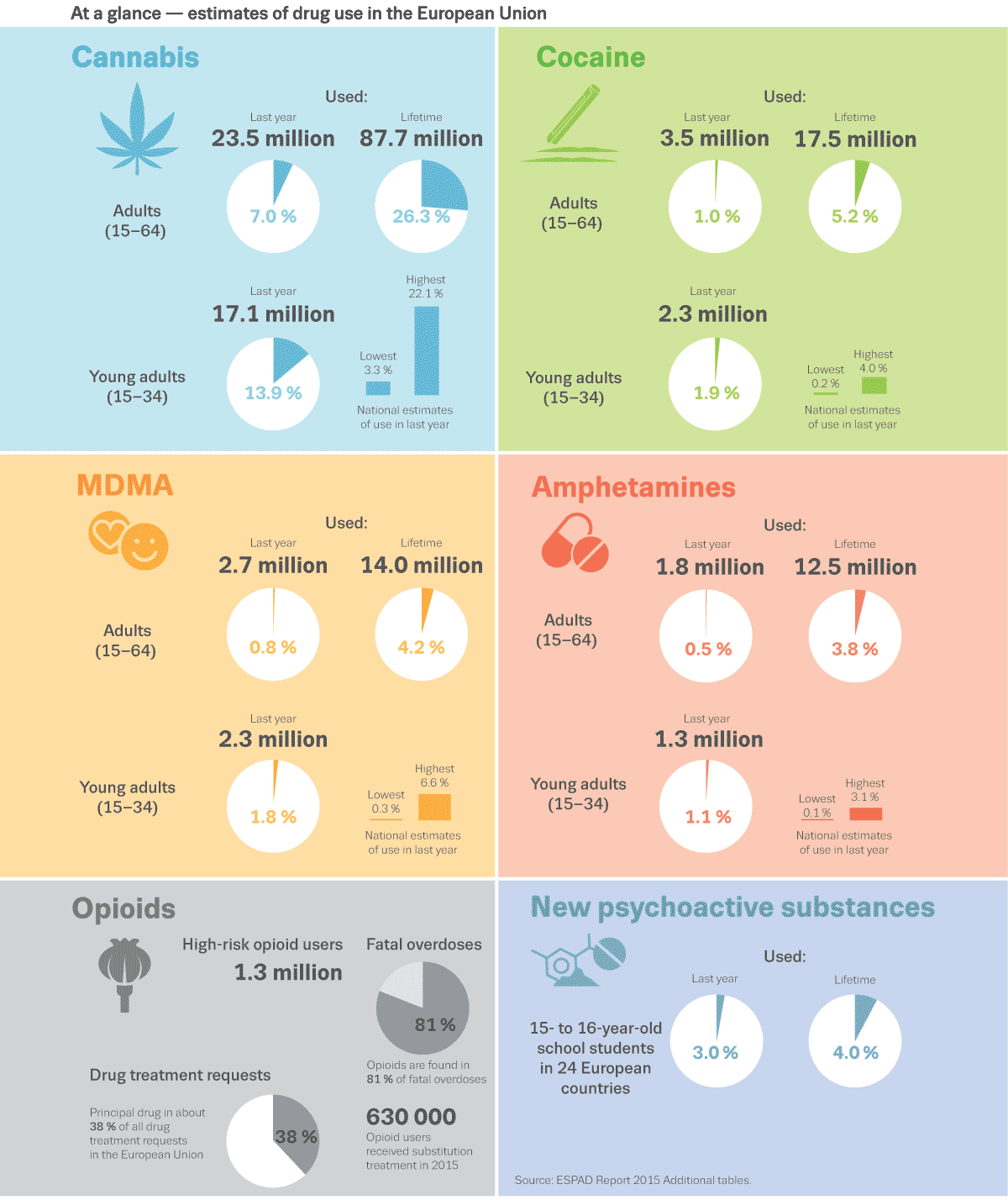
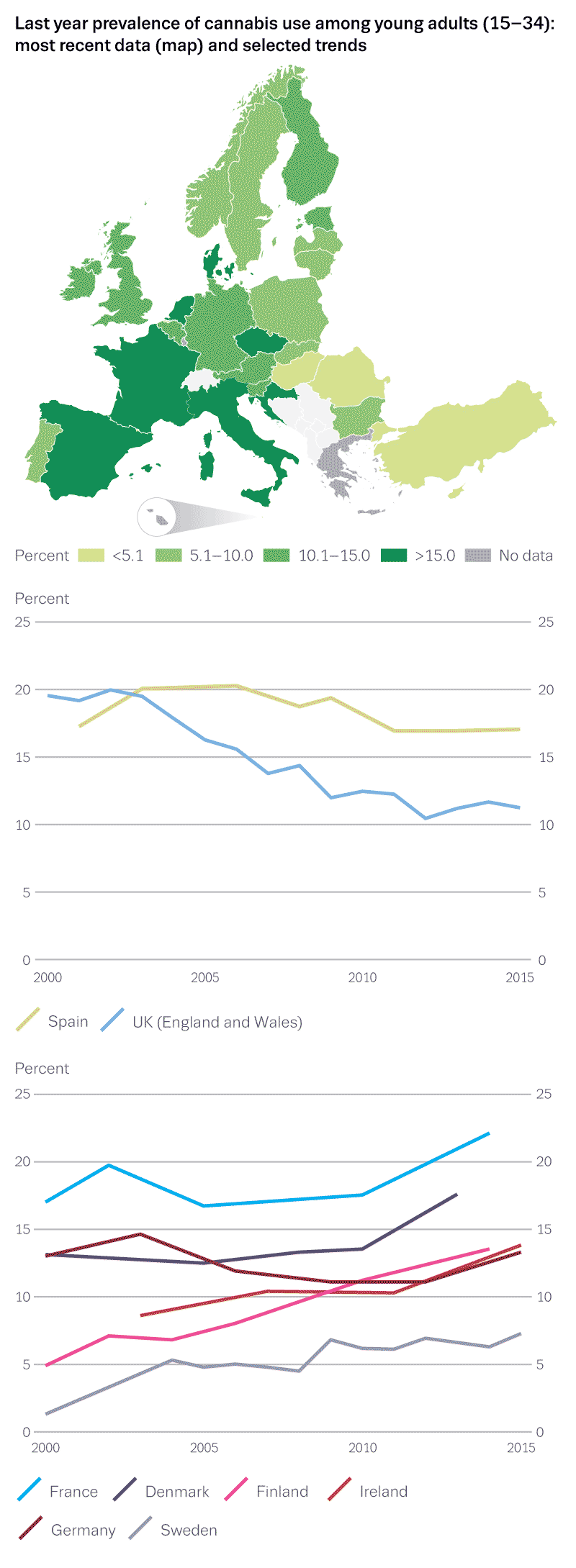
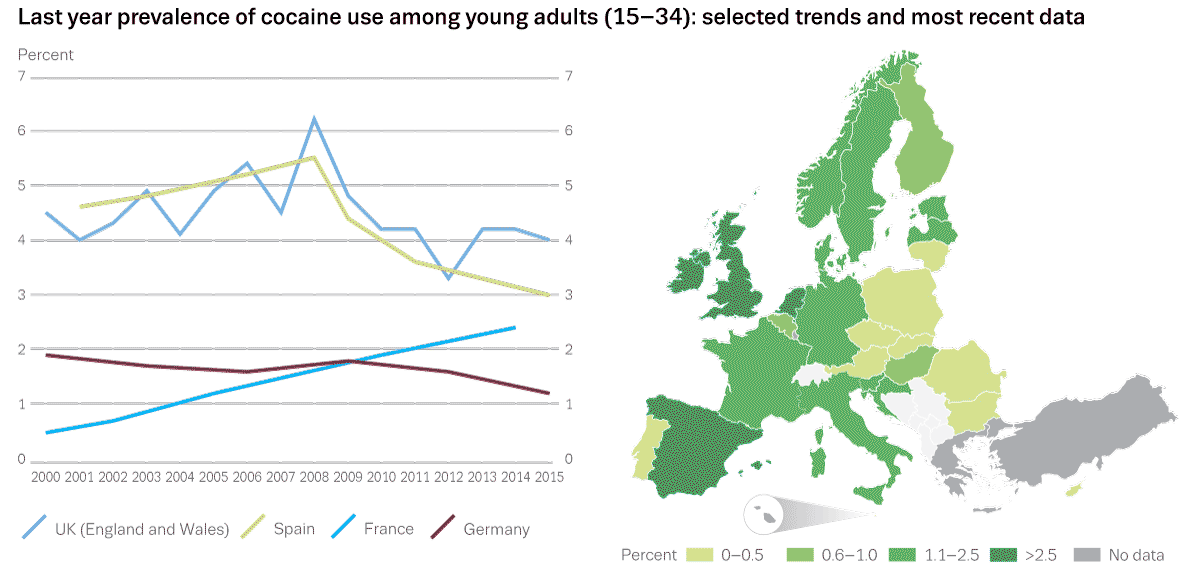
The adult population that is surveyed using the GPS is defined as inhabitants aged 15–64 (sometimes called ‘all adults’). ‘Young adults’ is the subgroup of the general population aged 15–34.
The prevalence estimates of surveys are based on standard periods of time. The standard recall periods for illegal drugs are:
-
any use during the person’s life — lifetime prevalence, also called lifetime experience;
-
any use during the previous year — last 12 months prevalence, also called recent use;
-
any use during the previous month — last 30 days prevalence, also called current use.
For further definitions please see the GPS Handbook and the data collection template (see ‘Key links’ below).
Methods
General population surveys are conducted at the national level, and their core part generally follows the methodological guidelines developed by the EMCDDA in order to improve the comparability of population surveys in the EU. These guidelines include a set of common core items, additional voluntary modules and basic methodological recommendations. The set includes basic prevalence measures and use patterns of certain legal and illicit substances, basic socio-demographic characteristics, and opinion and risk perception questions. Questions about the drugs market and drug policies are considered optional. Countries collect the data within different survey contexts (e.g. health, drugs and alcohol, crime, social). Thus the questionnaires typically include various other questions. Data on the core items are then reported to the EMCDDA through an online data collection system called Fonte (see the link to the data collection template, in the ‘Key links’ below).
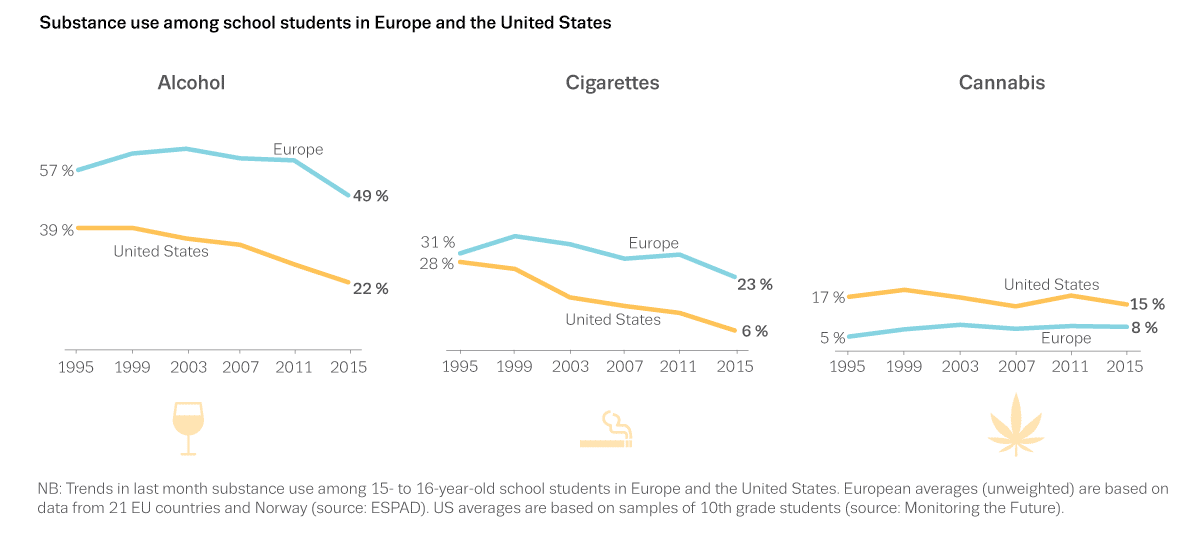
For information on surveys among school children see the section on ‘Methodology of school surveys’ in the Statistical Bulletin.
Data on targeted surveys within nightlife, universities and other settings are monitored for information on particular or intense drug use. This type of data is generated from studies and is therefore less harmonised.
Limitations
Given the nature of the surveys described above, a number of simplifying assumptions should be considered when using or quoting the resulting estimates:
-
The prevalence levels derived from a country’s general population survey are a reasonable estimate of the prevalence for the country and can be applied to the country population as a whole, provided the survey samples are representative of the population. Caution is required when non-response is non-random.
-
It is a reasonable assumption that the estimates of prevalence at the country level are comparable over time, allowing trends to be constructed, provided the survey methodology has remained constant over time. If the EMCDDA knows that a substantial change in method has occurred, the data is not used in trends analysis.
Limitations of the presented data include:
- Comparative analysis between countries should be made with caution, in particular where differences are small. Caution is required due to differences in survey methodology, mainly in survey context, data collection methods and sampling procedures. However, in the absence of a working alternative surveys do provide an indication of the scale of use. It should be acknowledged that there are limitations of surveys in estimating prevalence of the more intensive forms of drug use (e.g. heroin injection, crack use) due to the low prevalence figures, but in particular due to non-probabilistic errors (exclusion from the sampling frame, absence in household, non-response) and therefore cannot be used to obtain reliable estimates of the prevalence of these forms of use. The problem drug use (PDU) indicator provides estimates of the prevalence of, for instance, opioid use and injecting drug use to complement the GPS.
- In the case of adults, but even more so in the case of youth, the age ranges used to report results might have an influence on the results of prevalence estimates. Most countries use the EMCDDA-recommended age ranges (see above). However, different age ranges are occasionally used. If wider age ranges are used (e.g. 12–75 years) prevalence estimates tend to be lower because illegal drug use is relatively low at older ages. If narrower, younger age ranges are used (e.g. 18–49), estimates will tend to be higher because drug use is concentrated among young adults.
- The behaviours that are investigated retrospectively have the limitations of self-reports (concealment) and memory biases when survey participants are recalling past events.
- Countries conduct national surveys at different time intervals (years and months). The dates of the surveys should be considered when making comparisons between countries.
- Basic information on the survey methods adopted by each country has been compiled to aid interpretation. This includes the context, the sampling frame, the response rate of the most recent survey and other relevant information. Cross-referencing with EMCDDA and other data collections is recommended.
Key links
For further information please refer to the following:
- Handbook for surveys on drug use among the general population
- The GPS web page
- National reports
- Data collection template
- National methods and definitions — forthcoming. Awaiting final validation.
- Youth and schools surveys: methods and definitions
(1) The EMCDDA publishes a detailed Handbook, which includes the European Model Questionnaire (EMQ), holds annual meetings of both experts and data providers, provides direct assistance to data providers, and monitors and reviews the academic literature. Further information is available on the EMCDDA website (see ‘Key links’).